No products in the cart.
You shift onto your side and the shooting pain at the front of your pelvis makes you wince out loud. Getting out of the car took three tries this morning. Putting on your jeans meant sitting on the bed. Your midwife said it is common. You are 32 weeks in and wondering what is going on.
Pelvic girdle pain (PGP) is one of the most common pregnancy complaints women don’t talk about much. It is painful, it is frustrating, and it is treatable. At Inform Physio in Fairfield and Carlton, pregnancy pelvic pain is something we see every week in pelvic health physiotherapy sessions. Many of the women we see have been told, in one way or another, to put up with it. That is rarely the right answer.

What is pelvic girdle pain?
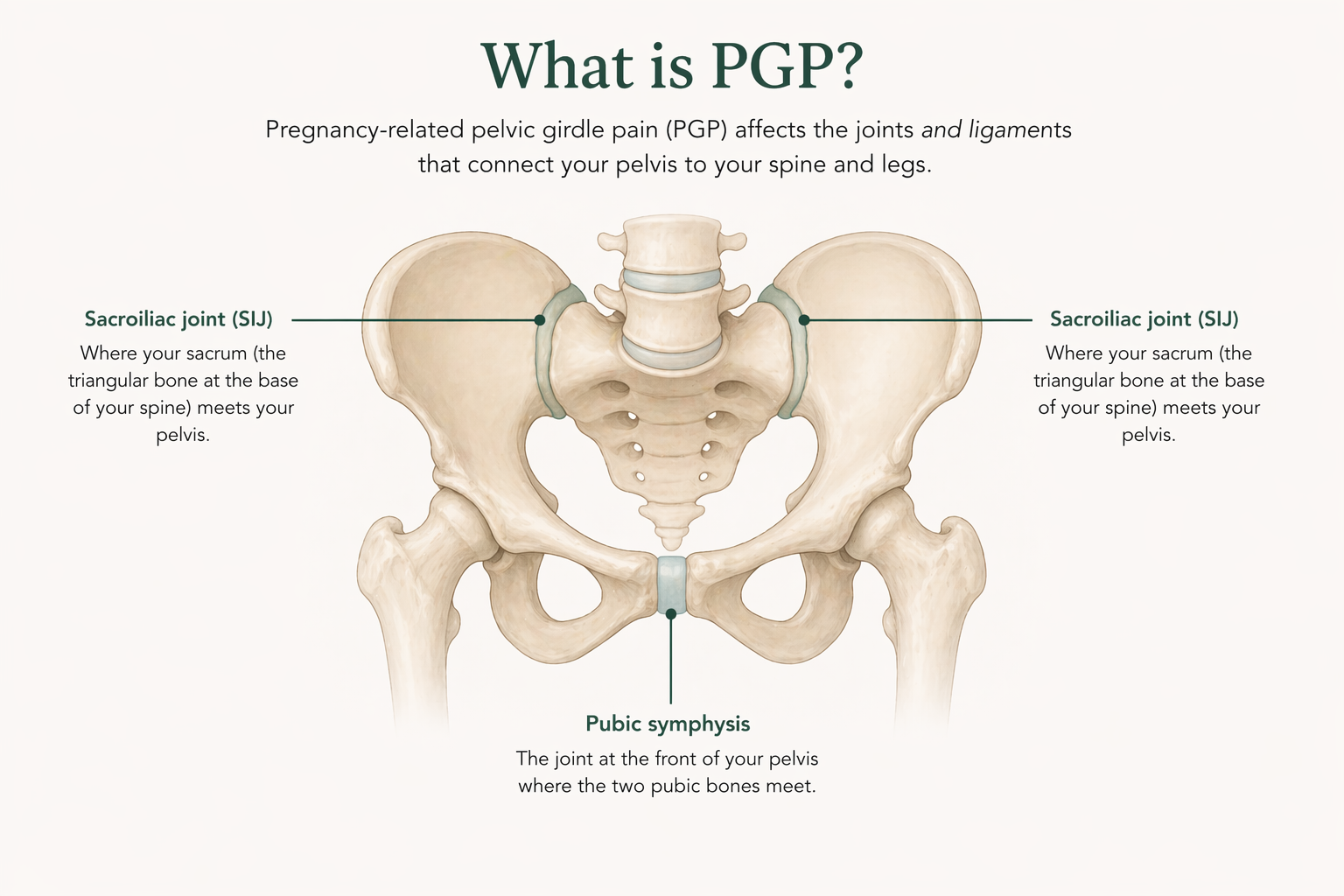
PGP is pain around the pelvic joints during pregnancy. It can affect the front of the pelvis at the pubic symphysis, the back at one or both sacroiliac joints (the dimples above your bottom), or both. The older term symphysis pubis dysfunction (SPD) is still used by some clinicians. The current clinical term is pelvic girdle pain.
The mechanism is more complex than a single hormone. For many years, pregnancy PGP was blamed on relaxin loosening the pelvic ligaments. Evidence has shifted that picture. The Pelvic, Obstetric and Gynaecological Physiotherapy network in the UK notes that studies have found no consistent link between relaxin levels and pain. The pelvis stays strong and stable through pregnancy. What drives the pain appears to be a combination of altered loading as your baby grows, changes in how the pelvic joints transmit force, individual stability patterns, and the nervous system’s pain response.
Who tends to get pelvic girdle pain?
A systematic review in the European Spine Journal reported prevalence ranging from roughly 4 per cent to 90 per cent across studies, with a mean of around 45 per cent. A 2024 meta-analysis in Acta Obstetricia et Gynecologica Scandinavica put pooled lumbopelvic pain in pregnancy at about 63 per cent. Around one in five women have pain severe enough to affect daily life.
Some women are at higher risk than others:
- Prior low back or pelvic pain. The single most consistent predictor.
- A previous pregnancy with PGP. Recurrence in later pregnancies is common.
- Multiple pregnancies. Risk tends to increase with parity.
- Hypermobile joints. Conditions where joints stretch more than usual are linked with higher risk.
- Physically demanding work. Heavy lifting, prolonged standing, or repetitive twisting through the day.
- A higher BMI before pregnancy. Additional load on an adapting pelvis.
You can still develop PGP without any of these. They are risk factors, not prerequisites.
What does pelvic girdle pain feel like?
The hallmark of PGP is pain that flares with specific movements and eases with rest. Most women describe some combination of:
- Sharp or grinding pain at the front of the pelvis, around the pubic bone.
- Deep, stabbing or aching pain in one or both sacroiliac joints at the dimples of your lower back.
- Pain that radiates into the groin, inner thigh, or buttocks.
- Pain with turning over in bed, getting in and out of the car, standing on one leg, or walking up and down stairs.
- Pain that worsens through the day, after a long walk, or after a period of prolonged standing.
- A clicking, grinding, or feeling of giving way in the pelvis.
PGP is not caused by damage and will not harm your baby, according to Royal College of Obstetricians and Gynaecologists patient information. It is, however, a clear signal that the load through your pelvis is outpacing the stability you have available right now. That is where physiotherapy can help.

When is it not pelvic girdle pain? Red flag symptoms
A small number of pregnancy pelvic symptoms are not PGP and need urgent review. If you have any of the following, contact your maternity team the same day or present to your hospital’s birth suite:
- One-sided shooting pain down the leg with numbness, weakness, or pins and needles that does not settle with position changes.
- Any loss of bladder or bowel control, difficulty emptying your bladder, or numbness around the saddle area (the skin between your legs).
- Any vaginal bleeding or reduced fetal movement.
- Severe sudden-onset pelvic pain that came on out of nowhere and is not relieved by rest.
- Severe one-sided groin pain with difficulty putting weight on that leg, particularly in the third trimester.
These symptoms are rare. When they happen, they are not things to wait out.
What you can do yourself to ease the pain
Simple changes often take the edge off. They do not replace assessment, but they help many women feel better quickly:
- Sleep with a pillow between your knees. Keep your top knee in line with your hip, and keep the pillow in place when you turn.
- Move as one block when rolling over in bed. Squeeze your knees together and turn as a unit rather than letting your top leg fall forward.
- Get in and out of the car with your knees together. Sit down first, then swing both legs in together. A plastic bag on the seat helps you pivot.
- Avoid standing on one leg. Sit down to put on underwear, trousers, shoes, and socks.
- Take stairs one step at a time. Lead with the less painful leg going up and the more painful leg going down.
- Skip breaststroke in swimming. A flutter or dolphin kick is fine. The frog kick loads the symphysis directly.
- Stand with your weight evenly on both feet rather than resting on one hip.
What can physiotherapy do?
A pelvic health physiotherapy assessment for PGP identifies which joints are involved, how your pelvis is transmitting load, and where stability is falling short. The 2015 Cochrane Review by Liddle and Pennick (the most recent at the time of writing) found that tailored physiotherapy combining exercise, manual therapy, pelvic support, and advice can reduce pain and improve function in pregnant women with PGP.
Treatment at Inform Physio usually includes:
- Manual therapy to ease muscle tension and gently mobilise stiff joints around the pelvis and lower back.
- An individualised exercise program for the deep core, gluteal muscles, and pelvic floor. These are the muscles that support the pelvis under load, and the program is adjusted as pregnancy progresses.
- Activity and movement retraining. Simple changes to how you move can reduce pain significantly, particularly for car transfers, rolling in bed, and stairs.
- A non-rigid pelvic support belt where indicated. Some women find a belt genuinely helpful, others do not. We fit and trial before recommending one.
- Guidance on birth positioning. If PGP is severe, planning ahead with your maternity team about positions that keep your knees close together during labour can make a real difference.
Physiotherapy does not remove the pregnancy, which is the underlying driver of PGP. What it aims to do is reduce pain, keep you moving, and help you stay active and comfortable in the weeks leading up to birth.
Does pelvic girdle pain resolve after birth?
For most women, yes. PGP typically settles within weeks to a few months of delivery as hormones return to baseline and the mechanical load reduces. A 2016 longitudinal study in BMC Pregnancy and Childbirth found that around one in ten women had ongoing PGP up to 11 years later. If your pain is not settling within three months of giving birth, a pelvic health physiotherapist can assess what is keeping it going.
Frequently asked questions
In most cases yes, though the type often needs to change. Supported, symmetrical movement (swimming without breaststroke kick, stationary bike, walking within a pain-free distance) is usually fine. Avoid running, heavy squatting, and single-leg loading. A physiotherapist can tailor exercise to your stage of pregnancy.
Yes, in most cases. Let your maternity team know about your PGP so they can support your legs during labour, help with position changes, and keep your knees close together where possible. Caesarean section is not routinely recommended for PGP (per the Royal College of Obstetricians and Gynaecologists) and may slow recovery.
PGP in a previous pregnancy is a significant risk factor for recurrence. Working on pelvic floor, core, and hip strength between pregnancies can reduce severity and make management easier from the start of the next pregnancy.
No. Private physiotherapy does not require a GP referral. Some women come with a referral under a Medicare Chronic Disease Management plan, which may offer a partial rebate. Most private health funds provide rebates under extras cover.
Yes. Pelvic health physiotherapy is appropriate at any stage of pregnancy. Later in pregnancy the assessment and treatment positions change (side-lying rather than lying on your back, for example), but the treatment itself is safe and commonly done.
Book a pregnancy physio assessment at Fairfield or Carlton
If pelvic girdle pain is keeping you from sleeping, walking, or getting out of the car without dread, you do not need to wait it out. A pelvic health physiotherapist can identify which joints are involved, give you strategies that work from day one, and adjust the treatment to the stage of pregnancy you are in. Initial pregnancy physio appointments run for 60 minutes. To book, or if you are not sure whether your pain is PGP, get in touch with our Fairfield or Carlton clinic.