No products in the cart.
You have had painful periods since they started. Maybe since your early teens. You have been told it is normal, or told it is bad luck, or told to try the pill. Maybe you have had a laparoscopy. Maybe you have a diagnosis of endometriosis. Maybe you do not. Either way, the pain has kept going, and now a GP or a specialist has suggested pelvic physiotherapy. You are wondering how that could possibly help, because this does not feel like a muscle problem.
Fair question. Physiotherapy is not a cure for endometriosis, and it does not replace medical or surgical care. What it does address is one specific piece of persistent pelvic pain: the muscle and nervous-system changes that build up in response to years of pain, and that often keep pain going even after hormonal treatment or surgery has done its part. At Inform Physio, our pelvic health physiotherapists see this pattern regularly, at both the Carlton clinic and the Fairfield clinic. This article explains what pelvic physiotherapy can help with, what it cannot, and where it sits in the broader management of endometriosis and persistent pelvic pain.

What is endometriosis, in plain terms?
Endometriosis is a condition where tissue similar to the lining of the uterus grows in other parts of the body, often within the pelvis. It causes inflammation, scarring and pain, and can affect fertility. The condition is common. According to Endometriosis Australia and the Australian Institute of Health and Welfare, around 1 in 7 Australian women, girls and those assigned female at birth are estimated to live with endometriosis.
This article is not meant to be a full endometriosis resource. For a comprehensive overview of the condition itself, Endometriosis Australia is the authoritative Australian reference. The focus here is on what happens after diagnosis, or after years of suspected but unconfirmed endometriosis, when pain persists despite medical treatment.
Why does endometriosis pain often persist after medical treatment?
This is the question that makes pelvic physiotherapy make sense.
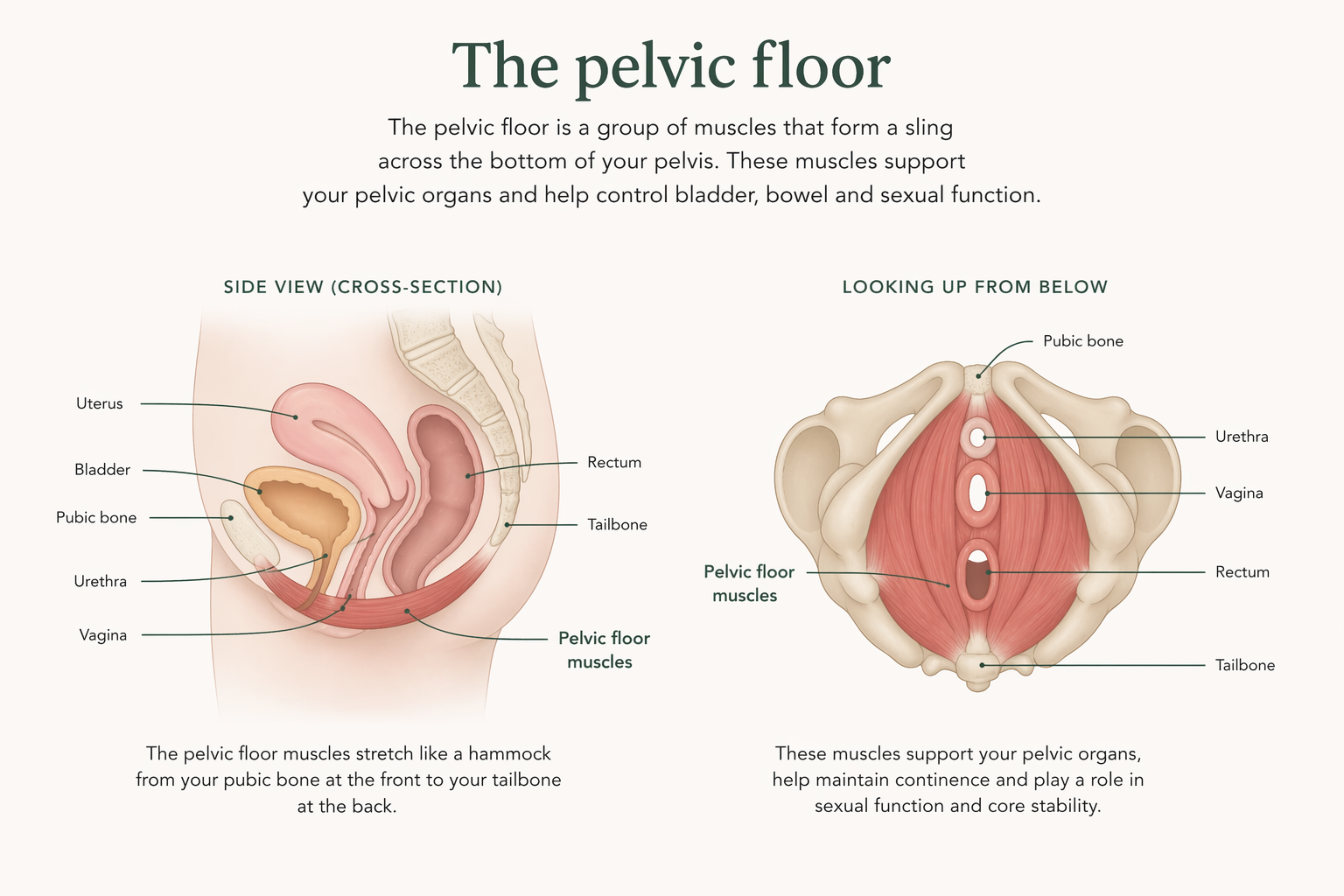
Pain that continues for months or years changes how the body responds. The pelvic floor muscles, which sit at the base of the pelvis and support the bladder, bowel and uterus, are protective by design. When there is pain in the area, these muscles tighten. The tightening is a protective response that happens automatically, without conscious choice.
Over time, if the pain keeps coming, the pelvic floor can stop fully relaxing. This pattern is sometimes called an overactive or hypertonic pelvic floor. A pelvic floor that is always on carries a noticeable ache of its own, and makes normal activities like sitting, intercourse, bowel movements and inserting a tampon painful or difficult. The original source of pain may have been endometriosis lesions, but the ongoing pain is now substantially driven by the muscles themselves.
The nervous system also adapts. Nerves that carry pain signals from the pelvis become more sensitive with repeated activation. The brain learns to interpret pelvic sensations as painful at lower thresholds than before. This process is called central sensitisation, and it is well recognised across chronic pain conditions. It helps explain why pain can continue even when hormonal treatment is working and surgery has removed visible lesions.
The practical consequence is this: a significant portion of the pain that persists after medical treatment is muscular and nervous-system driven. And that part responds to pelvic physiotherapy.
What happens at a pelvic pain physiotherapy assessment?
The first appointment is mostly talking. Your physiotherapist will take a detailed history, often for 30 minutes or more, covering your pain pattern, medical and surgical history, menstrual history, bladder and bowel function, sexual function where relevant, and the impact on daily life. This history itself is part of the clinical work. The pattern of the pain often points clearly to what is contributing.
Assessment then typically includes looking at your posture, breathing, abdominal muscle activity, and how you move. For many people, this is where the first appointment ends.
An internal vaginal examination is sometimes offered because it gives the most direct information about the pelvic floor muscles, but it is not compulsory. It is only performed with your informed consent, and only when it would meaningfully change the treatment plan. You can decline, defer, or revisit it at a later appointment. Plenty of useful treatment can start without one.
Education is a significant part of the first appointment. Understanding how chronic pelvic pain works is one of the more effective pain-reduction tools available, and it is free of side effects. Expect to leave with a clearer map of what is going on, and a small starting plan.
What does treatment involve?
Treatment is individualised, but common components include:
- Manual release of overactive pelvic floor muscles. Hands-on techniques to help tight pelvic floor muscles let go, either externally through the lower abdomen and hips, or internally where appropriate and consented to.
- Down-training exercises. Learning to actively relax the pelvic floor. This can feel counterintuitive if you have spent years being told to do Kegels, but for persistent pelvic pain the treatment priority shifts toward teaching release.
- Bladder and bowel retraining. Pelvic pain often affects bladder frequency, constipation and pain with bowel movements. Simple changes to emptying strategy and toilet positioning often help.
- Breathing and nervous-system work. Paced diaphragmatic breathing, vagal stimulation techniques, and graded exposure to normal sensations help calm a sensitised nervous system.
- Gradual return to activity and exercise. Many women with persistent pelvic pain have stopped moving because movement hurts. A staged return, often through clinical pilates, can rebuild confidence without flaring pain.
Treatment is cumulative. Few people feel resolved after one session. Meaningful change usually starts to show across a handful of appointments, and longer-standing pain patterns generally take longer to settle.
Where does physiotherapy fit in a multidisciplinary team?
Pelvic physiotherapy is one piece of care. Endometriosis and persistent pelvic pain are complex conditions that usually respond best to a team approach.
The Australian Government's National Action Plan for Endometriosis, released in 2018, established multidisciplinary care as a national priority. The Australian Living Evidence Guideline: Endometriosis, developed by the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) and updated in 2025, includes specific recommendations for physiotherapy and psychological interventions as part of standard care.
A typical team may include a GP with an interest in pelvic pain, a gynaecologist, a pelvic health physiotherapist, a pain specialist, a psychologist experienced in chronic pain, and sometimes a dietitian for endometriosis-related gut symptoms. Not everyone needs every professional, and the mix shifts over time. The Pelvic Pain Foundation of Australia is a useful national resource for understanding the full range of options.
Physiotherapy works alongside medical and surgical care, not in place of it. If hormonal treatment or surgery is being considered or is underway, pelvic physiotherapy runs in parallel, and often becomes more effective once medical management has stabilised the underlying condition.
A quiet note on getting here
Many women arrive at pelvic health physiotherapy having been told for years that nothing was seriously wrong, or that the pain was just period pain, or that they should learn to live with it. Diagnostic delays for endometriosis in Australia have averaged several years, though an Australian survey published in Scientific Reports in 2020 suggested the delay is reducing as awareness grows.
A good pelvic health physiotherapist starts from the position that the pain is real and treatable. You do not need a definitive endometriosis diagnosis to benefit from treatment. You do not need a referral. You do not need to have tried anything specific first. If pelvic pain is affecting your life, that is reason enough to book.
Frequently asked questions
No. You can book directly. If you have a chronic disease management plan from your GP, up to five allied health sessions per year may be Medicare-subsidised, but a referral is not required to start. Private health extras typically cover pelvic physiotherapy, depending on your level of cover.
No. An internal examination is only done with your informed consent, and only when it would add useful information to your treatment plan. A detailed history and external assessment are usually enough to start. The examination can be deferred, declined, or revisited later, and treatment can progress regardless.
Treatment should not cause sharp or lasting pain. Some hands-on work can feel tender, particularly if the pelvic floor is very tight, but your physiotherapist will work within what you tolerate, and will pause or stop at your request. Managing pain flares is part of the clinical approach, not a sign that something has gone wrong.
This varies. Some people notice meaningful change within three to four sessions, others need ongoing care over several months. Your physiotherapist should give you an honest estimate after the first assessment, and reassess the plan regularly. Longer-standing pain patterns generally take longer to settle.
The pelvic floor and nervous-system changes that develop with persistent pelvic pain look similar regardless of underlying cause, so the treatment approach overlaps substantially between endometriosis, adenomyosis and IBS-related pelvic pain. Polycystic ovary syndrome does not typically cause pelvic pain directly, but if you have pelvic pain alongside PCOS, the assessment looks at the pain mechanisms rather than the hormonal condition.
Booking a pelvic health assessment in Carlton or Fairfield
If you are weighing up whether to book, know this: the first appointment is structured to give you as much control as possible. Nothing invasive happens without your informed consent, and plenty of useful treatment can begin with a conversation and an external assessment. Bringing a partner, parent or friend into the room is welcome if it helps.
Inform Physio runs pelvic health physiotherapy from both the Carlton clinic, convenient for inner-north and CBD residents, and the Fairfield clinic, which serves the inner-north-east. You can book online or call the clinic to arrange an initial assessment. If you are unsure which location suits, the reception team can help you choose based on appointment availability and travel.